Today, there are many educational materials and support groups for people with dwarfism. We also live in a society that respects and can adapt to the physically challanged. This begs the question: is treatment really necessary?
Anybody less than 5 feet tall will quickly discover that society was not built with them in mind. Everyday items in our homes, such as door knobs, coat racks, light switches, seat height and depth, toilet seat height, freezer doors, and shower controls, are designed around an expected height. Medicine today allows us to adapt the individual to the environment. How do we help achondroplastic individuals adapt to their environment? We can alter their stature. Spinal growth is not affected to the same extent as limb growth in individuals with achondroplasia; they have a relatively normal trunk. This is why limb lengthening works as a treatment. It restores body proportions.


Primary goal of treatment: increased height
At the Paley Orthopedic & Spine Institute, we believe that lengthening for dwarfism should be available to those who want it. Ultimately, it is a patient and family decision. It is not something that must be done. Patients should be aware of all the risks and benefits. Anyone interested in lengthening of this nature needs to be careful to have it done at specialized centers with extensive experience, in order to ensure a successful outcome. Four-segment lengthening at the Paley Orthopedic & Spine Institute can be done safely, reliably, and reproducibly.
Treatment Goals
The goals of treatment for patients with achondroplasia are to:
- Achieve increased height
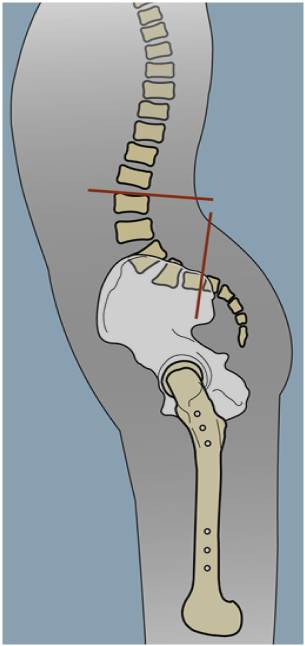
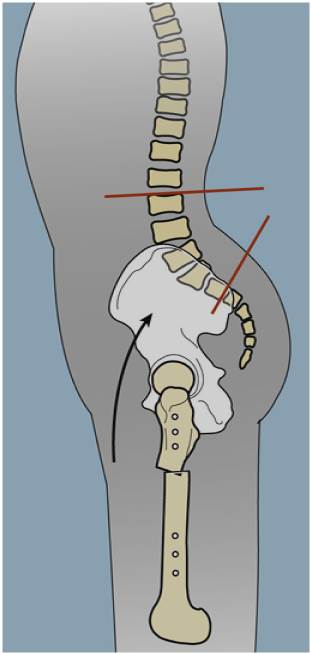
- Correct hyperlordosis of the spine
- Correct bowleg deformity
- Improve reach
- Restore body proportions
- Preserve patient function
Correct Hyperlordosis
Correct Bowleg Deformity


Treatment consists of extensive limb lengthening of the femurs, the tibias, and the humeri. For more information on limb lengthening and the biology of distraction, see the Limb Lengthening Center. Treatment strategies for more complex dysplasias differ and will be discussed elsewhere.
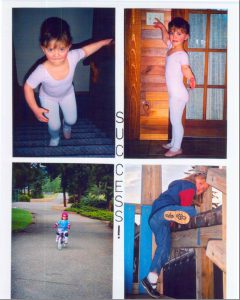
Ultimate Goal: Restore Patient Function


Treatment Schedule
Surgical treatment aims to correct the upper and lower limb deformities while simultaneously increasing stature. This typically results in leg lengthening between 30 cm and 40 cm for the average patient with achondroplasia. Lengthening of the lower extremities can be as high as 15 cm per session; thus a total of two to three leg lengthening sessions are required. The upper extremity is lengthened via the humerus, which is lengthened separately from the leg.
8–10 years old
- Both tibias: 4 cm
- Both femurs: 6 cm
- Total length gained: 10 cm (~4”)
13 years old
- Both tibias: 7 cm
- Both femurs: 8 cm
- Total length gained: 15 cm (~6”)
14/15 years old
- Both humeri: 10 cm (if undergoing 2 lengthenings of lower extremities)
- Both humeri: 12 cm (if undergoing 3 lengthenings of lower extremities)
- Total length gained: 10 cm (~4”) or 12 cm (~4.7")
16 years old
- Both tibias: 7 cm
- Both femurs: 8 cm
- Total length gained: 15 cm (~6”)
- Total stature gain: 40 cm (~16”)
Ideally, the first lengthening would be performed between the ages of 8 and 10. If you start lengthening too much too early, there is a risk of growth inhibition. For this reason, we will not lengthen younger than age 8. The first lengthening is also conservative. We will simultaneously lengthen both femurs and both tibias 4 cm per bone for a total of 8 cm of length. The average external fixation treatment time is five months.
The second lengthening occurs at 13 years of age. If the patient did not have the opportunity to lengthen during childhood, the first lengthening can be performed at this time. Once again, a simultaneous lengthening of both femurs and both tibias will be performed and any deformities of the lower limbs corrected at this time. Length achieved is usually between 10 to 15 cm and the average external fixation treatment time is five to seven months.
The next lengthening will be a lengthening of the upper extremities, typically around 14 years of age. Both humeri are lengthened between 10 and 12 cm, dependening on the number of lower extremity lengthenings. If 3 lower extremity lengthenings are undergone, we will lengthen the humeri up to 12 cm in order to maintain proportion.
The fourth lengthening will occur between the ages of 15 and 16 and is a third lengthening of the lower extremities. Once again, both femurs and tibias are lengthened simultaneously for a total length gain of 10 to 15 cm. We will correct any remaining deformities: flexion deformities of the hips (this corrects the lumbar hyperlordosis), any femoral varus or valgus, and any residual tibial deformity. Average external fixation time is five to seven months. A fifth and final lengthening can be performed, if needed, at 17 to 18 years of age.
Childhood activities are easily possible in between the lengthenings. In fact, the lengthenings improve the patient’s ability to engage in age-appropriate activities.
By lengthening the arms between the two leg lengthenings, the legs receive a well-needed break from lengthening. Most patients report that the arm lengthening is significantly easier and does not get in the way of normal activities.
The minimal time between lengthenings is generally at least 6 to 12 months after the device is removed. The advantage of lengthening both femurs and tibias simultaneously is that the total external treatment time is reduced significantly. Furthermore, this approach allows for maximum height gain in the shortest time. The disadvantage of bilateral simultaneous femoral and tibial lengthenings is increased nursing care and physical therapy involvement.
Skilled, daily physical therapy is an integral part of the treatment program for achondroplasia. As such, our patients are required to relocate to our vicinity during the distraction (lengthening) phase of treatment. When the patient enters the consolidation phase, they are allowed to return home to continue physical therapy. Typically the consolidation time is roughly the same duration as the distraction time. The patient will have limited to very light weight-bearing and will be wheelchair bound untitl there is adequate bone healing towards the end of the consolidation phase. At the end of consolidation, the patient returns to our center for fixator removal.