The abundance of literature suggests that if treatment is commenced prior to age 4, Blount’s disease can be reversible. This is because a growth arrest or physeal bridge has not yet occurred.
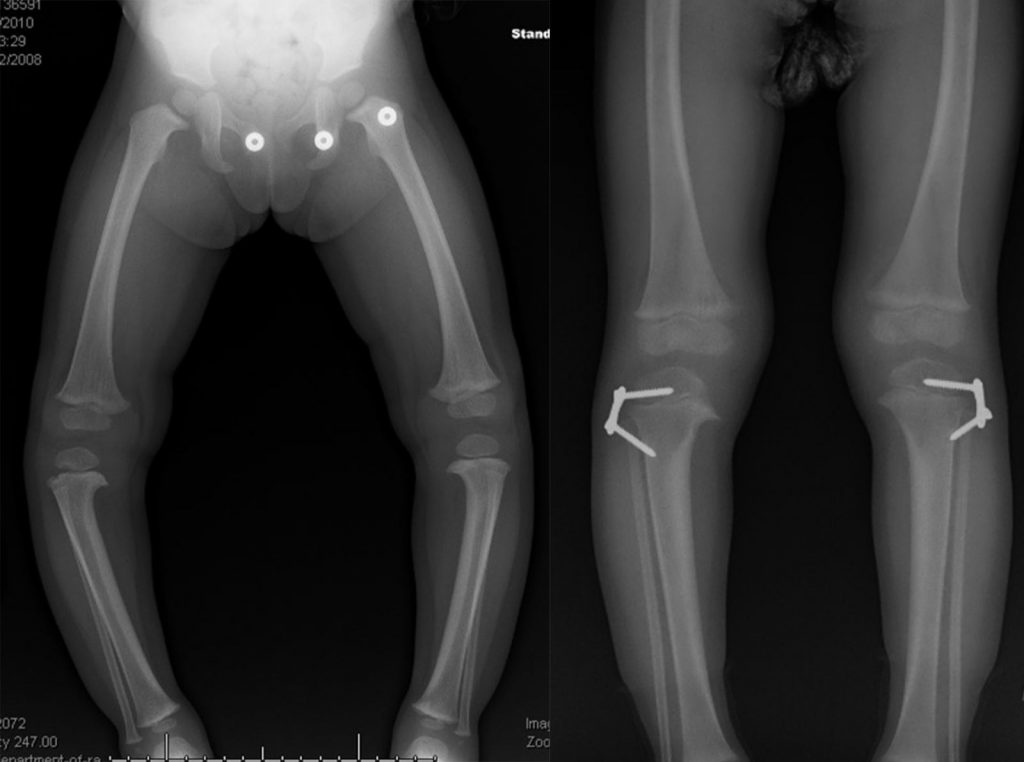
A variety of braces have been designed for Blount’s disease to try and correct the bow leg deformity. Most of these have now been abandoned and replaced by the early use of hemi-epiphysiodesis with screw plate devices. At the Paley Institute, our preference once Blount’s disease has been diagnosed is to perform the hemi-epiphysiodesis. This is a minor outpatient procedure in which small metal staples are inserted in one side of the growth plate of the upper tibia. This procedure temporarily tethers the growth on the outside of the tibia forcing the leg to grow straight; this process is also referred to as guided growth. Hemi-epiphysiodesis requires vigilant follow up to track the growth correction. Once the leg is straight, the metal staples will need to be removed so that the leg will then continue to grow straight. Failure to properly track correction may result in over-correction and a resultant deformity in the opposite direction (knock knee deformity).
The other alternative is osteotomy. At this young age, a metaphyseal osteotomy of the upper tibia below the tibial tuberosity combined with lateral translation and external rotation of the tibia is very efficacious to correct the deformity. While the hemiepiphysiodesis plates are useful for correcting the varus deformity they do not address the rotational deformity. Osteotomy can address both. It can also be performed bilaterally simultaneously. If it is performed gradually with an external fixator, no fasciotomy is required while it is performed acutely an anterior compartment fasciotomy is advisable.