Children born with fibular hemimelia have a spectrum of deformity, deficiency, or instability (DDI). The surgical treatment for fibular hemimelia is designed to address all of the deformities, deficiencies, and length discrepancies, specific to each type and the individual patient’s needs. At the Paley Institute, we start with a reconstructive life plan. This involves evaluating all of the surgical deformities, deficiencies, and predicting the limb length discrepancy at maturity and then coming up with a surgical plan to correct these in the fewest number of surgeries, spread apart as much as possible throughout the child’s growing years.
The goals of treatment are to achieve the following by skeletal maturity:
- Equalized limb length
- A functional foot in the plantigrade position (flat on the ground)
- Alignment of the hip, knee, and ankle joints
- Knee stability.
For more details on treatment, see Dr. Paley's article in Journal of Children's Orthopedics: Surgical Reconstruction for Fibular Hemimelia

Reconstructive Life Plan
A reconstructive life plan for fibular hemimelia may look like this:
SUPERankle Surgery and First Lengthening
- 5 cm of length gained
- Performed age 18 - 24 months
Second Lengthening
- 5 - 8 cm of length gained
- Performed age 7 - 10
Third Lengthening
- 5 - 8 cm of length gained
- Performed age 12 - 14
Epiphysiodesis ("8 plate")
- 5 cm of length gained
- Performed around age 9 for girls and age 13 for boys
Total length gained: 15 - 30 cm (6 - 12 inches)
The first step for treatment is to predict the limb length discrepancy at skeletal maturity. During the initial visit with Dr. Paley, he will obtain x-rays of both lower limbs and measure the lengths of both femurs, both tibias, and the heights of both feet. By comparing the sum of the femur, tibia, and feet height on the short leg with that on the long leg, we can determine the limb length discrepancy at the time of the x-ray. Using the multiplier method for limb length discrepancy prediction (a formula developed by Dr. Paley in 2000), we can calculate the limb length discrepancy at skeletal maturity. Additional measurements throughout the patient’s life will improve the accuracy of the prediction.
Once the predicted limb length discrepancy at skeletal maturity has been calculated, a determination on the number of limb length equalization surgeries can be made. Under the age of four, it is safe to lengthen up to 5 cm (~2 in.). As the patient ages, subsequent lengthenings can be as high as 8 cm.
If additional equalization is required, one can also consider a limb growth-slowing procedure, called an epiphysiodesis. The epiphysiodesis involves slowing the growth of the long leg to allow the growth of the short leg to catch up and equalize. While limb lengthening can be performed at any age, an epiphysiodesis has to be performed at a very specific age in order to achieve a specific amount of growth slowing. We rarely use epiphysiodesis to achieve more than 5 cm (~2 in.) of limb length equalization. This covers the majority of cases of fibular hemimelia. In rare cases with larger discrepancies shortening of the femur or simultaneous lengthening of the femur and tibia may be preferred.
Fibular Hemimelia Classification
The next step will be to determine the type of fibular hemimelia. At the initial consultation, it is determined whether the patient has a fixed foot deformity (or even a dynamic foot deformity) that will require surgical treatment. Fibular hemimelia is classified into different groups dependent on treatment strategies according to the degree of severity. Many different classification systems have for FH have been proposed, but these systems have historically prioritized amputation treatment.
In 1995, Dr. Paley developed a classification for fibular hemimelia that takes reconstruction into account. The Paley classification divides fibular hemimelia into four groups: types 1, 2, 3, and 4. It further subdivides Type 3 into four subtypes: 3A, 3B, 3C, and 3D. The method of treatment is specific to each type and subtype:
- Type 1 – stable ankle joint
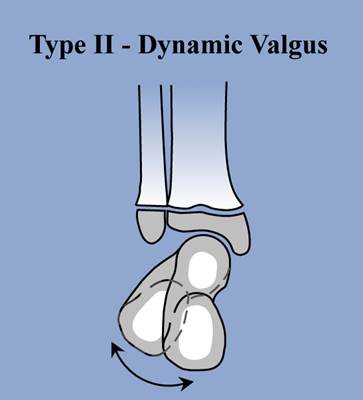
- Type 2 – valgus deformity of the foot
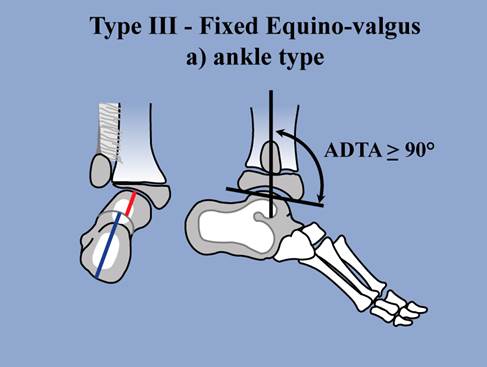
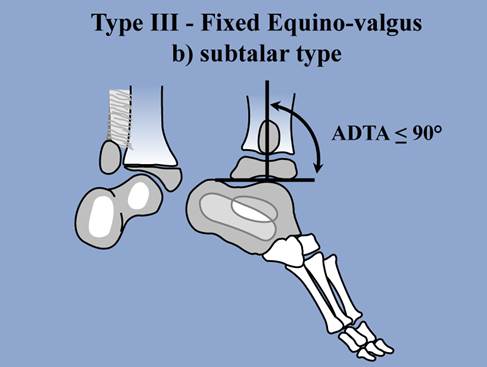
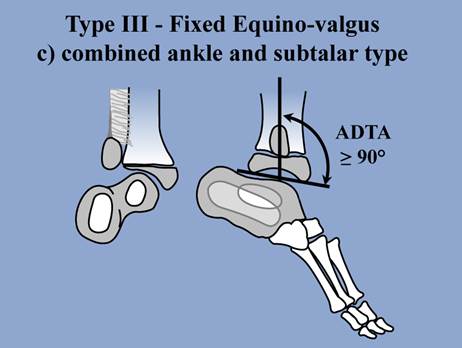
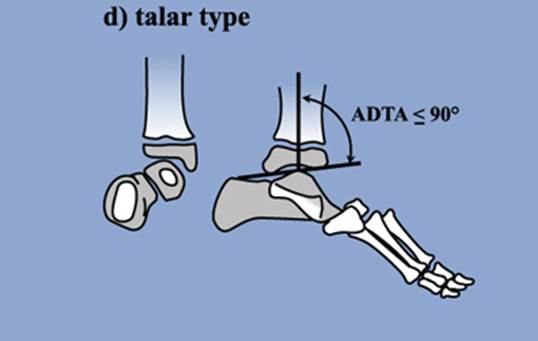
- Type 3 – equinovalgus deformity of the foot
- 3A – equinovalgus due to malorientation of the ankle joint
- 3B – equinovalgus due to malunited subtalar coalition
- 3C– equinovalgus due to combination of malorientation of ankle joint and malunited subtalar coalition
- 3D – subtalar deformity other than a subtalar coalition
- Type 4 – equinovarus deformity of the foot (also known as “clubfoot type”)
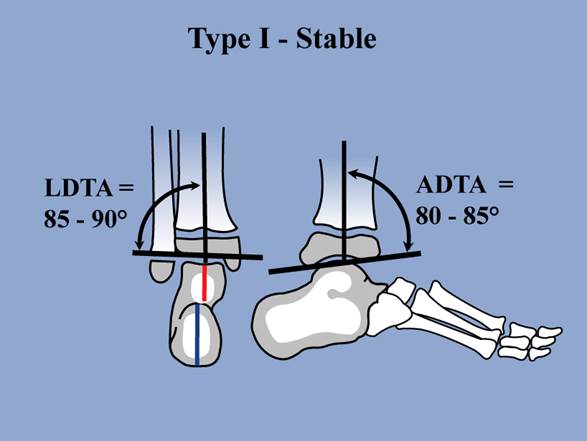
Paley Type 1 is a congenitally short tibia and fibula with a stable ankle joint. In many cases, the ankle of Type 1 cases appears completely normal and the fibula is only slightly shorter at its upper end compared to the opposite side. The predicted limb length discrepancy in Type 1 cases is typically less than 7 centimeters (3 inches). Type 1 FH is also referred to as the Stable type due to the stable ankle joint. Most patients with Type 1 do not require any foot surgery. In many of these cases, lengthening of the tibia and fibula will address the deformity.