When bone breaks, it naturally regenerates to fix the fracture. Lengthening works by separating the bone and distracting (pulling apart) the bone segments very slowly so that new bone continues to form in the gap. As the bone segments are slowly distracted, the bone regenerates, resulting in increased length.

For more information on the science behind limb lengthening and the development of lengthening techniques over the last 25 years, see Progress in and from Limb Lengthening
See also this article on Deformity Correction by the Ilizarov Technique
The device that performs the lengthening is called a fixator. Dr. Paley uses a variety of fixators and they can be divided into two categories: the external fixator and the internal fixator or implantable lengthening nail.
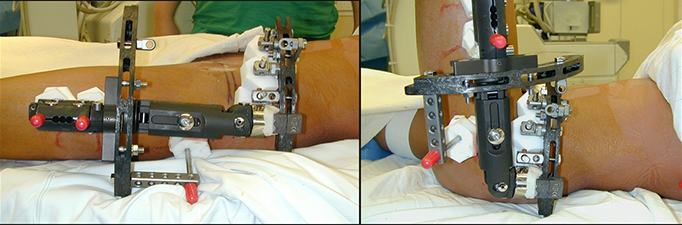
External fixators are devices that attach to the bone through wires and pins. The external fixator looks and acts like a scaffolding, supporting the separated bone. The fixator mechanically lengthens the limb by pulling the segments of bone apart. There are two types of external fixators: monolateral (e.g. the Modular Rail System) and circular (e.g. Ilizarov device and Taylor Spatial frame).
Internal fixators or intramedullary nails can also be used for lengthening. Dr. Paley currently uses the PRECICE 2, a modification of the original PRECICE which was FDA-approved in 2011. The PRECICE is an internal telescopic rod that is implanted inside the marrow cavity of the bone. The device lengthens similar to the way an antenna extends. An external remote control is used to rotate a magnet inside the nail. This in turn rotates gears which turn a drive screw, which extends the telescopic nail.
The lengthening process is divided into two phases: distraction phase and consolidation phase.
Lengthening Surgery

During the lengthening surgery, an osteotomy is performed. An osteotomy is a surgical cut of the bone. Once the bone is separated, the fixator is applied.
After surgery, most patients stay in the hospital for two to three days and inpatient rehabilitation begins the day after surgery. This includes teaching the patient to get out of bed, move their joints, use a walker or crutches, transfers to the chair and toilet, and the use of stairs.
Lengthening will begin a few days to a week after surgery. The time after surgery and before the lengthening begins is known as the latency period. It is necessary to wait a few days before lengthening so that the callus (new bone) can form at the break site.
Lengthening is done manually with the external fixator and the rate is approximately one millimeter (mm) per day, but may be slower or faster depending on the tolerance of the bone and soft tissues. To make the lengthening gentler, the one millimeter per day is broken into quarter millimeter increments. Parents and patients are taught to turn the distraction rod on the external fixator one quarter turn (1/4 mm) four times per day. Lengthening with the PRECICE is done using an external remote control (ERC) device. During the first week, our orthopedic technologists train the patient, family, and caregivers on how to use the ERC device.
Distraction Phase

The distraction phase is the actual lengthening of the bone and is also known as the lengthening phase. During this period, the external or internal fixator will gradually lengthen the bone approximately one millimeter per day.
Patients typically begin outpatient physical therapy following discharge from the hospital. Therapy is a critical component of the lengthening process and is required every single day. Most patients do therapy five days a week (Monday through Friday; weekend therapy available in some cases) and do home exercises with their parents and caregivers on weekends. Families are instructed on how to perform home exercises.
For more information on physical therapy at the Paley Institute, see Center for Rehabilitation & Physical Therapy.
Compliance with home therapy is crucial to a successful lengthening outcome. The more therapy the patient receives, the better the functional result and faster the rehabilitation after removal. Most parents and caregivers can become excellent therapists.
Physical therapy during lengthening is very different from other orthopedic surgeries. After most orthopedic procedures, the patient is at their worst following surgery and gradually recovers. In lengthening, the patients are at their best one week after surgery. As their bones are distracted, the muscles become tighter and tighter and range-of-motion of joints becomes limited. In this sense, it may appear that the patient gets worse as they lengthen.
Once the patient has concluded lengthening and begun the consolidation phase, the normal pattern of recovery resumes. It may be helpful to consider the lengthening process as a continuous surgery, one that does not conclude until the desired length is achieved.
Consolidation Phase
Once the patient has reached their desired length, they enter the consolidation phase. No further adjustments are made to the fixator. The fixator will remain until the end of the consolidation phase to allow the newly-formed bone to harden. The total time in the external fixator can be estimated to be approximately 1 month for each centimeter of lengthening in children and 1.5 to 2 months (or longer) per centimeter for adults. Total fixator time is divided evenly between the distraction and consolidation phases.
Most patients stay in West Palm Beach during the distraction phase and prepare to return home during the consolidation phase (we usually recommend staying at least two weeks after the end of the distraction phase). Physical therapy continues through the consolidation phase. Bone healing is followed using x-rays obtained once a month. If the patient has returned home, x-rays are obtained locally and emailed or mailed to Dr. Paley. When Dr. Paley has assessed that the bone is sufficiently healed, the patient returns for fixator removal, a minor outpatient surgical procedure.
For more information, please see our video on the Biology of Limb Lengthening and our video on Limb Lengthening Methods
Deformity Correction
There are a variety of deformity correction techniques that Dr. Paley performs to correct deformities of the bones, joints, and soft tissues. Many of these techniques can be performed in conjunction with limb lengthening.
Epiphysiodesis
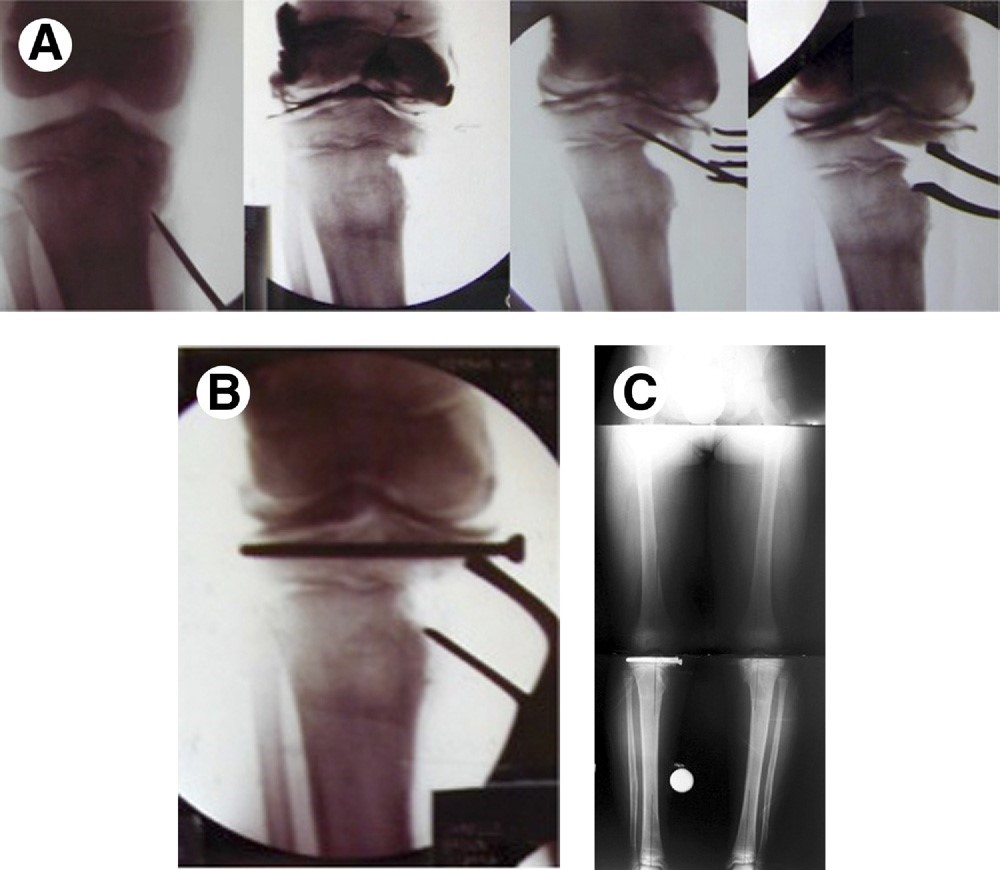
An epiphysiodesis is a minor outpatient procedure in which small metal staples are inserted into the growth plate of a long bone (e.g. tibia). This procedure temporarily tethers the growth of the bone. In an epiphysiodesis, both sides of the growth plate are tethered, which completely halts growth. This can be used as an alternative to limb lengthening to correct a limb length discrepancy; halting growth on the long leg will allow time for the short leg to "catch up" and equalize limb length.
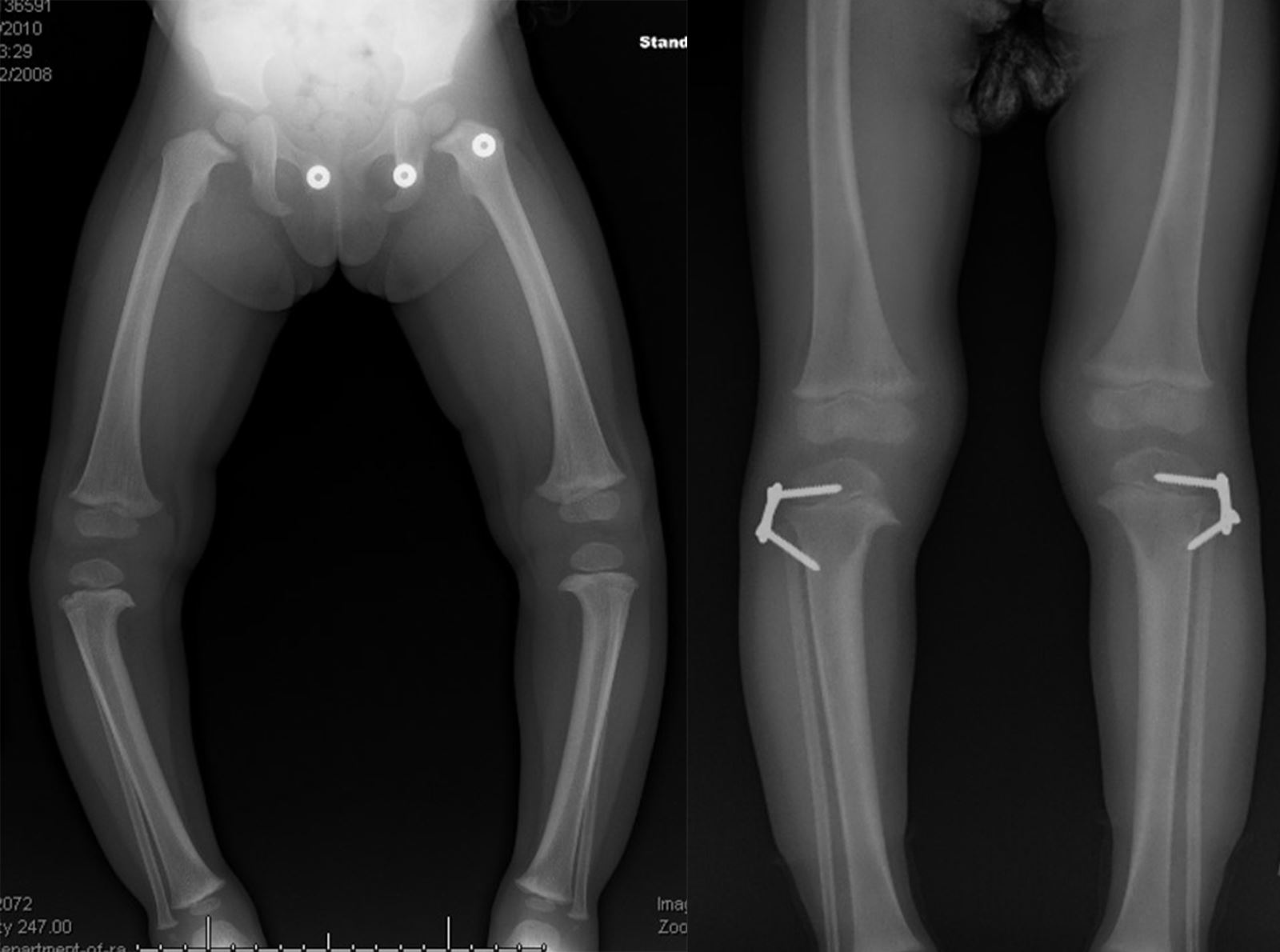
A hemi-epiphysiodesis is a technique in which only one side of the growth plate is tethered. This halts growth on one side but allows growth on the other side, allowing for gradual angular correction. This approach is often used to correct varus (outward) and valgus (inward) deformities of the knee. For example, if a patient has varus deformity, their knees bow outwad By performing a hemi-epiphysiodesis on the outside of the growth plate, the deformity will gradually correct as the patient grows.
Epiphysiodesis is a gradual approach. Correction is achieved slowly and may take several years. Since the procedure relies on an open growth plate, it is only viable in children who are still growing.
Osteotomy
An osteotomy is a surgical cut to the bone. It is used to separate bone during limb lengthening. Osteotomy can also be used for limb deformity correction with or without lengthening. Osteotomy is used to realign bones and joints by performing a cut at the apex of the deformity. The bones and joints are then reoriented into the proper alignment and stabilized with internal or external fixation. An intra-articular osteotomy is an osteotomy performed within a joint (e.g. the knee) and an extra-articular osteotomy is performed on the bone, outside the joint.
Intra-articular osteotomies are used in Joint Preservation techniques.
Osteotomy followed by limb lengthening can be used to treat highly complex limb deformities. Dr. Paley uses the Taylor spatial frame (TSF), a specialized external fixator that uses a computer program to gradually correct limb deformities in a three-dimensional space. In addition to lengthening the bone, the TSF can also gradually straighten the bone as well.

Dr. Paley has developed many specific osteotomies to correct complex limb deformities. He is also the author of The Principles of Deformity Correction (Springer-Verlag, 2002), a textbook that has set the standard for the understanding and treatment of limb deformities.
Distraction
Distraction is a technique used to correct joint contractures. A contracture is stiffness or constriction of the joint resulting in reduced range of motion (ROM) and function. The technique uses an external fixator which is attached to the bones surrounding the joint (e.g. the femur and tibia for a knee contracture). The fixator then gradually distracts (pulls apart) the joint, slowling lengthening the tightened muscles and tendons in the joint, correcting the contracture.
Distraction is also be used in the treatment of Perthes Disease and Hip AVN. The hip joint is distracted in order to reduce pressure on the collapsed femoral head.