TREATMENT
Dr. Dobbs uses The Ponseti Method to treat clubfoot. This method is the most common treatment in the U.S. and consists of serial casting, heel cord tenotomy, brace wear, and stretching. The treatment goal is to have a well functioning, pain-free, and normal foot. Treatment typically consists of 5 casts with a tenotomy on the 5th cast.
PHASE 1
Casting: Casting can begin when the baby has reached seven pounds and the foot is as long as the parent’s pinky finger. The cast is changed every 7½ weeks to gently stretch and reposition the foot and extends from the groin to the toes. An accelerated casting option is available where casting occurs every 4 days to expedite the process. The outcome is the same as the traditional weekly casting.
You are with your baby during casting and may comfort them with a bottle, pacifier, or any method of distraction. Your baby may be fussy during casting but it is not painful. Only the clubfoot is stretched and casted. They may be sensitive to the heat and wetness of the plaster. Prior casts are removed with a cast saw by ortho techs who are highly skilled at cast removal on babies.
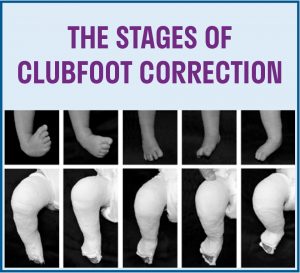
The image below shows the gradual correction obtained in each cast
WHEN YOU GO HOME IN CASTS
Toes: Support the cast at all times to prevent slipping. While the cast is on, you will make sure the toes are pink and always visible. If the toes disappear in the cast, it must be removed. Contact us for instructions on how to remove the cast. It is normal for the toes to be somewhat cool and dusky for the first 24 hours but will pink up later in the day or the following morning.
Bathing: In order to keep the cast clean and dry you will give your baby sponge baths. Wrap the cast in a towel to keep it dry during bath time.
Sleeping: Roll up a towel, blanket, or small pillow and put it under the cast. This will help support the feet and legs and make your baby more comfortable.
Diaper Changes: Change diapers often to make sure nothing leaks onto the cast. Keep the diaper area covered at all times while changing. Use a wet wipe to clean the cast when necessary. The top of the cast should be outside of your baby’s diaper.
Clothing: Buy clothes a size or two larger than normal. Wide-legged pants, stretchy pants, loose-fitting leggings, and elastic waistband pants work well. Leg warmers or long socks will protect the cast from diaper leakage. Gowns work well at bedtime.
Skin irritation: If the cast rubs at the top of the thigh you can use Moleskin, Coban, foam tape, and/or a leg warmer or long sock to pad the area.
When to contact the doctor:
- If the toes disappear in the cast
- If toes are dark and cold regardless of repositioning
We encourage you to email pictures or Facebook message Dr. Dobbs if you are concerned about either of these problems.
PHASE 2
Tenotomy: The Achilles tendon is clipped to lengthen the heel. This procedure is typically done in the clinic with local anesthesia in children under a year of age. Parents are present at the bedside for all casting appointments. Parents are asked to wait in the waiting room during the tenotomy due to the sterility of the procedure. You will be given instructions at the appointment prior to the tenotomy
Before application of the final cast, the baby is measured for the brace and will have a minor procedure to lengthen the Achilles tendon. Dr. Dobbs performs the tendon lengthening procedure in the clinic under local anesthesia. You may offer your child Tylenol before the procedure and for the first 24 hours after the procedure. Check with your pediatrician for the correct dosage. Please have a bottle and pacifier ready for us to offer during the procedure. You may keep your baby on their normal feeding schedule.
On that day you will:
- Have the cast removed
- Get measured for the brace system so it will be ready at your next appointment
- Wait in a separate room during the procedure and casting
- Stay for 30 minutes after we bring your child back to you so we can make sure there is no bloodstain on the back of the cast
- Make your 3-week follow-up appointment
You may see a bloodstain appear on the back of the cast at the ankle area. This stain can appear throughout the first day. It will be about the size of a quarter. Blood should NOT seep out of the cast or come around the front of the cast by the toes. Please contact us immediately if this should occur.
When you return in 3 weeks the casts come off and the brace goes on. Please bring tight, long socks to this appointment.
PHASE 3
Bracing: When the final cast is removed, your child is placed in a foot abduction brace designed to prevent the clubfoot deformity from recurring. The brace will be worn 23 hours a day for three months, 18 hours for the next three months, 14-16 hours for the next three months, and 12-14 hours a day (naps and nighttime) until your child is 4 years old. The goal is to be in nap and night time wear by the time they are pulling up.
After the last cast comes off, your child goes immediately into the brace. Bracing keeps the foot in the correct position. The feet are typically rotated to 60-70 degrees but may be set at a different level upon Dr. Dobbs recommendation. This is not uncommon for those with complex clubfoot or underlying neurological conditions.
Clubfoot will relapse if the brace is not worn. It is absolutely necessary that the brace be worn 23 hours a day for three months. We then wean down to 18 hours for the next three months, 14-16 hours the next three months, and then recommend 12-14 hours a day (naps and nighttime) until your child is 4 years old.
Braces will not delay your child’s development when it comes to sitting, crawling, or walking. NOT wearing the brace will compromise the correction of the clubfoot. The braces need to fit correctly like shoes and will go up in size as your child grows. It is important to remember that this is a new and different situation for your baby. Your baby may be fussier than normal because this is not something they are used to, but braces are not painful.
WHEN YOU GO HOME IN BRACES
Expect your baby to be fussy while getting used to the brace. Be relentless! The brace is not painful however it is new and different and can be very frustrating for you and your child. You will all adapt to the brace just as you did to the casting process.
The next 3 months are full-time brace wear (23/24 hours per day).
The 1 hour per day your child is out of the brace can be divided into three 20 minute breaks or four 15 minute breaks throughout the day.
Remove the brace to:
- Give your baby a bath – do not use lotion on the feet (causes slipping)
- Check for blisters and skin breakdown
- Change socks if they are damp from sweating
- Do stretching exercises
The brace is to be worn tight to keep the feet from slipping and rubbing. If blisters develop you may need to leave the brace off to allow the skin to heal.
DO NOT remove the brace while the child is crying. Calm them before removing the brace so they learn that crying will NOT get the brace removed.
You will return to the clinic in one month for a brace check and then two months after that. At the end of three months of successful brace wear, you will be instructed on how to decrease the hours in the brace.
The hours will be gradually decreased to sleeping and non-active times. It is very important that the baby learns to sleep in the brace from day one.
Typically a child needs 2-3 pairs of boots the first year and 1 pair every year after that. This ultimately depends on the growth of the child.
Cleaning Braces: Mitchell shoes may be washed in the washing machine. Put boots in a pillowcase or mesh laundry bag. Wash with a cold, gentle cycle, with no soap and let air dry. Do not wash the bar in the washing machine.
Cotton socks are recommended.
Socks should not bunch, wrinkle, or be too big. A grip on the bottom will help to prevent the foot from slipping. You can cut the toes out
of the socks in warmer weather. Socks should cover wherever the boot touches. To prevent irritation from the seam in the toe, you can turn the socks inside out as long as they do not have grips on the bottom.
Blisters/Skin Irritation: Red marks, blisters, bruising, and pressure sores are common. If you are concerned a sore is infected, contact Dr. Dobbs by sending pictures via email or Facebook message. You can put corn starch or baby powder in the socks and use band-aids, moleskin, mole foam, lamb’s wool, or Duoderm on the sore. Pressure saddles from MD Orthopedics will relieve pressure on the top of the foot as well as sheepskin under the tongue. Do not use lotions or creams on red spots.
Cribs: Braces may hit the crib causing noise and damage. This may be reduced by using boot covers, bar bumpers, crib bumpers that cover the individual slats in the crib, and sleep sacks that may help with this. Go Mama Go Designs or Bumpsters sell crib slat covers or you can use pool noodles or pipe insulation.
Baby Wearing: The Beco Gemini carrier fits well in the brace stage, although many carriers will work. Take the bar off the boots and put back on when the baby is positioned correctly in the baby carrier. This is the same case when your baby sits in a high chair, a shopping cart, or a baby jumper.
Bar Covers: Padding the bar will help protect your child, yourself, your furniture, and siblings. Some suggestions are:
- Clubfoot Accessories (personalized): https://www.facebook.com/clubfootcover
- D-Bar Enterprises: http://www.dobbsbrace.com/bar-covers. html
- The Padalily: http://www.padalily.com
- Taz at Bar Bumpers (personalized): https://www.facebook.com/bar.bumpers.
- Foam pipe insulation wrapped in decorative duct tape
- Hand towel wrapped in decorative duct tape
- Luggage handle cover
- Pool noodle wrapped in decorative duct tape
- Seatbelt cover
- Leg warmers
Car seat: A standard car seat will work.
Shoes: Bare feet are best, but when wearing shoes, your child can wear normal shoes. It is common that clubfoot children have different sized feet.
Child Care: Talk to your child care provider about your child’s treatment.
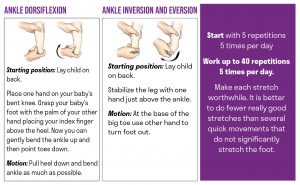
STRETCHING EXERCISES
Stretching, like bracing, is critical in maintaining the correction of your child’s feet.
ADDITIONAL MANAGEMENT
After three months of successful brace wear we monitor your child closely every 3 months for signs of recurrence. You may always contact us sooner if you are concerned or have brace issues. Our goal is that your child’s feet are flexible and in a good position for walking and running.