Ollier’s Disease is a condition where multiple enchondromas (benign tumors of cartilage) are found (usually asymmetrically) throughout the skeleton, leading to limb length discrepancies and deformities. Ollier’s leads to the second largest magnitude of limb length discrepancy after congenital femoral deficiency. Ollier’s Disease is quite rare, occurring in 1 in 100,000 individuals; it occurs more in males than in females. Ollier's Disease is a non-hereditary condition.
Other conditions associated with Ollier's Disease include:
- Multiple Hemangiomas - Maffucci's
- Intracerebral Gliomas
- Intracranial Chondroma
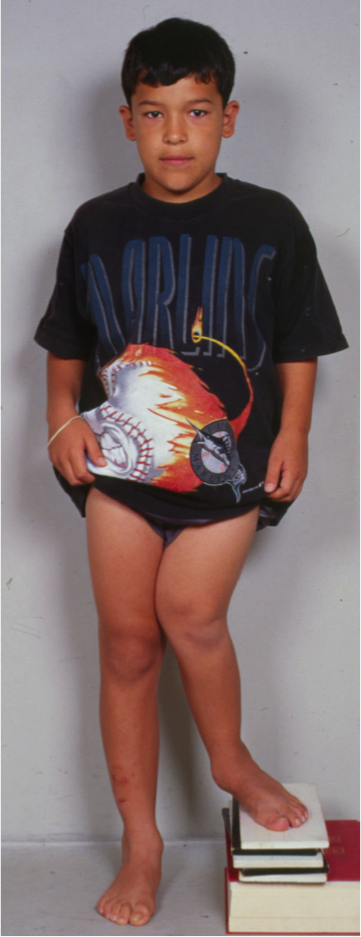
Limb length discrepancy (LLD) and angular deformity are two common orthopedic problems in patients with Ollier’s. The LLD is secondary to tethering of the growth plate by the enchondromas. Typically, there is predominance of involvement of one side. When Ollier’s is present on both sides of the growth plate, the most severe LLD and deformities result.
Angular Deformities
In the femur, the most common angular deformities are varus of the distal femur (inward at the knee) and valgus of the proximal femur (outward at the hip). In the tibia, the most common deformities are valgus of the proximal and distal tibia (outward at the knee and ankle). The valgus of the tibia is often associated or related to differential involvement of the fibula relative to the tibia. The fibula becomes shorter than the adjacent tibia leading to lateral tethering of the tibia with growth of the tibia into valgus at each end. At the knee, the proximal tibial valgus is often balanced by the distal femoral varus (lower femur bowlegged deformity balanced by upper tibial knock knee deformity). Since these two deformities effectively cancel each other out, there is often little knee malalignment despite deformity in both the tibia and femur.

The combined femoral and tibial deformity leads to a knee joint that is inclined relative to the ground (normally the knee joint line is horizontal, parallel to the ground). Fortunately, this inclination is a “good pattern.” The reverse inclination (valgus femur with varus tibia) is the “bad pattern.” Although correcting malalignment is important, uncorrected “good pattern” inclination does not usually develop into worse symptoms. “Bad pattern” inclination, however, leads to knee arthritis. Since Ollier’s patients typically display the “good pattern,” this is one of the explanations for why arthritis of the knee is uncommon in patients with Ollier’s Disease.
On the other hand, the inclination at the ankle (valgus of the distal tibia) is the “bad pattern” for that joint. The tibial valgus at the ankle joint combined with proximal (toward the knee) migration of the distal fibula leads to lateral subluxation (partial dislocation) of the talar joint. What this means is that the ankle bone (talus) moves out of place gradually as the ankle joint tilts to the side and the lower fibula moves upward, uncovering the outside of the talus. This deformity, if left untreated, leads to arthritis of the ankle joint later in life.
The other problem at the ankle is the recurvatum deformity of the distal tibia. This leads to further uncovering of the talus, resulting in increased risk of arthritis. As a consequence, an equinus contracture of the ankle develops (foot pointing downward). Therefore, correction of the recurvatum must be performed in coordination with correction of the equinus.
In addition to lower limb deformities, occasional upper limb deformities deserve surgical attention. In particular is the upper humeral deformity. The upper humerus usually deforms into valgus and extension. Rarely are forearm deformities seen. In the most severely involved Ollier’s case, finger deformities may be present and will require treatment.
Limb Length Discrepancy
Lower limb length discrepancy in patients with Ollier’s disease progresses proportionally. Since it is usually not present at birth, it is called a developmental (as opposed to congenital) discrepancy. Such discrepancies in children can be predicted at skeletal maturity. At the Paley Institute we use the Paley Multiplier Method to predict final limb length discrepancy. This allows us to develop a reconstructive life plan to comprehensively address the patient’s deformities and LLD so that they end up with no deformity and equalized limbs at skeletal maturity.
In Ollier’s the LLD can range from 10 to 30 cm. This can be corrected with 1 - 3 lengthenings of the femur and tibia simultaneously along with epiphysiodesis when necessary. Epiphysiodesis is a minor outpatient procedure where small metal plates are inserted into the growth plate of the unaffected (longer) leg. This hinders the growth of the long leg, reducing the amount of leg required to reach equal limb length. Epiphysiodesis can only be used to correct ~5 cm of length and can only be performed prior to skeletal maturity. Since epiphysiodesis results in shortened height, it is not preferred in patients who are predicted to be relatively short. In these cases, it is preferable to do lengthening only for equalization.
Arm length discrepancy in the humerus can also be predicted and treated with lengthening surgery.