Treatment for growth arrest aims to correct any resultant deformities, as well as any limb length discrepancy (LLD) or short stature. Different treatment strategies aim to address different clinical problems associated with growth arrest. Some of those problems and the suggested treatment include:
Clinical Problem: Tethering of the Growth Plate
- Treatment: Bar Resection
Clinical Problem: Angular Deformity
- Treatment: Osteotomy (Surgical Bone Cut)
Clinical Problem: Limb Length Discrepancy (LLD)
- Treatment: Limb Lengthening and/or Epiphysiodesis
Clinical Problem: Short Stature
- Treatment: Limb Lengthening
Bar Resection
Bar resection is a surgical procedure that aims to re-establish growth after growth arrest by removing the “bar” the section of the growth plate that has prematurely closed. There are various factors that favor bar resection over other treatment approaches, including:
- Less than 25% of the growth plate is affected
- The growth arrest is peripheral (rather than central)
- The affected individual is young, with a lot of growth remaining (under age 10 for boys and age 8 for girls)
- Damage occurs in one of the faster growing growth plates (distal femur, proximal tibia, distal radius, proximal humerus)
- Damage caused by traumatic event (thus unlikely to recur)
Bar resection is a relatively minor procedure with a short healing time. The procedure is used to prevent the patient from developing angular deformities and limb length discrepancies. If the patient already has severe angular deformities and/or limb length discrepancy, alternative treatments should be considered (see below). The best time to perform a bar resection surgery is on a young patient who has not yet developed any deformity or LLD. This will allow growth to continue normally throughout childhood. The best results have been reported with bar resection of less than 25% of the growth plate. Resection of larger sections of the growth plate are plagued with high failure rates.

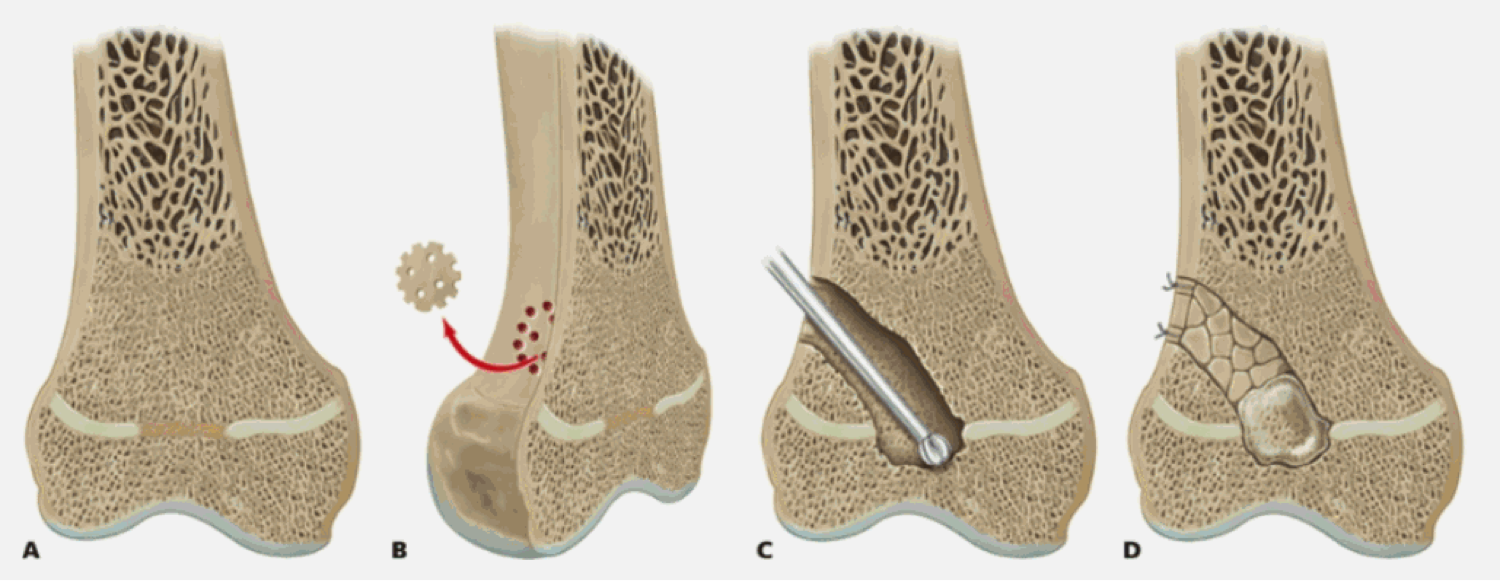
Surgical technique for bar resection involves the following steps:
- Map bar with MRI and CT scans
- Choose approach depending on peripheral or central arrest
- Choose interposition material (fat, cement, bone wax, autogenous chondrocytes, silicon, polytetrafurethylene, etc.)
- Insert metal markers to monitor growth after resection
Growth Plate Distraction
An alternative to the bar resection technique is to first distract the growth plate and then resect the bar through the open space. After the bar is resected, the interposition material is inserted. The major advantage to this approach is that it allows for deformity correction through the growth plate. Bar resection surgery does not correct a deformity, it only prevents them from occurring. By distracting the growth plate, the deformity can be simultaneously addressed. As in bar resection, this technique only works for younger children whose growth plates are normally open.
Epiphysiodesis
Epiphysiodesis is a gradual corrective technique that can be used on younger patients who are still growing. It is a minimally-invasive procedure that involves the insertion of small metal staples to one or both sides of the growth plate in order to impede growth. There are two approaches to epiphysiodesis:
- To prevent LLD - epiphysiodesis
- To complete partial closure - hemi-epiphysiodesis
If a patient has a growth arrest on one limb, an epiphysiodesis can be performed on the opposite limb to prevent a LLD from occurring. The unaffected limb will stop growing, and thus no LLD will occur. Keep in mind that this approach completely halts all growth. Epiphysiodesis is a surgically-induced growth arrest. Therefore, this approach is only ideal in patients who are close to skeletal maturity (and thus only a little bit of growth remains) and in those patients with whom stature is not a concern.
In a hemi-epiphysiodesis, only one side of the growth plate is affected. This approach is used to complete a partial closure of the growth plate and prevent angular deformities from occurring in younger children who are still growing.
Deformity Correction with Lengthening
Deformity correction in conjunction with limb lengthening can comprehensively address many of the problems that arise from growth arrest. Lengthening can correct LLD and short stature, and deformity correction can correct any resultant angular deformities. Furthermore, this approach can be used on patients of any age. This approach, however, is more invasive and involves significantly greater recovery time. Therefore, bar resection and epiphysiodesis are preferred in younger patients (under age 8 in girls and age 9 in boys).
Deformity correction and lengthening involves gradually correcting the deformity using an external or internal fixator. First, an osteotomy (surgical bone cut) is performed on the affected bone to break it into two segments. The fixator will then slowly distract (pull apart) the bone segments inducing new bone to form in the gap. This results in increased length. The fixator can also correct any angular deformities by gradually straightening the bone as well.
For more information, please see Limb Lengthening Center and the Center for Deformity Correction.
There are two approaches in growth arrest cases:
- Close the growth plate and then do osteotomy
- Distract the growth plate and then break the bar (method developed by dePablos)
Prior to lengthening, it is important to predict the the final limb length discrepancy. Dr. Paley developed the Multiplier Method to reliably predict LLD. In growth arrest cases, it is important to use the Developmental Formula and not the Congenital Formula.
Some patients may require stature lengthening when there is bilateral growth arrest, such as in meningococcemia. Bilateral lengthening can simultaneously correct any deformities and restore proportions and height.
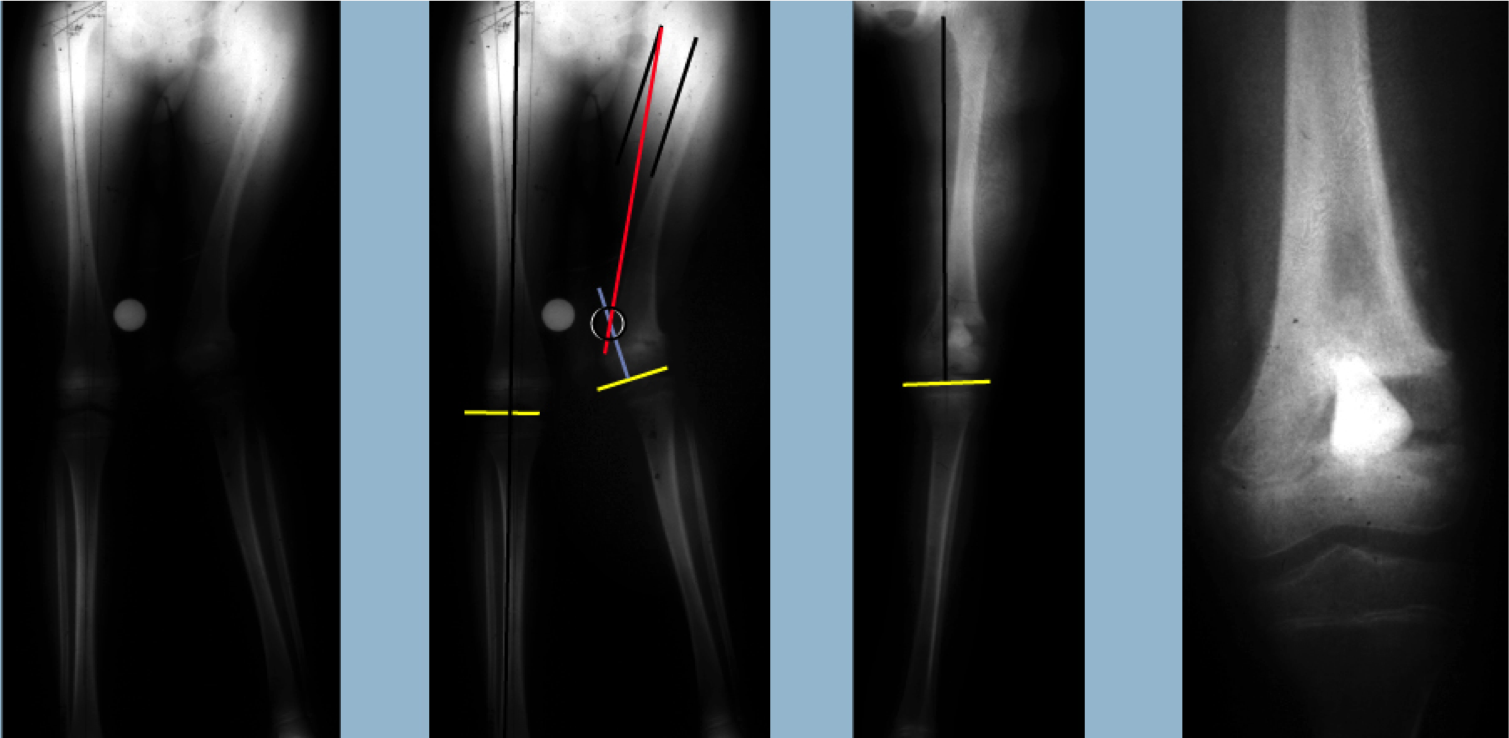
Patient Case Study: Post-Traumatic Growth Arrest w/ Lengthening & Osteotomy
Intra-Articular Osteotomies
Central growth arrest of the distal femur or proximal tibia often leads to incongruity of the knee joint. This results in various deformities inside the joint:
Plateau Depression
- Associated with Blount's Disease
Fishtail Deformity
- Associated with Neonatal Sepsis
Treatment for plateau depression involves a plateau elevation osteotomy. For more information, see Treatment Strategies for Blount’s Disease
Treatment for fishtail deformity involves osteotomies to split and realign the condyles. For more information, see Treatment Strategies for Neonatal Sepsis Sequelae
In each of these cases, the intra-articular osteotomies can be used to restore joint stability and congruity.
Growth arrest in Perthes can lead to misshapen femoral head with a saddle-shape deformity. A femoral head reduction osteotomy can be used to make the head spherical again. For more information, see Treatment Strategies for Perthes Disease
Conclusions
- Bar resection: use sparingly and only in younger children
- Osteotomy treatment: more reliable in correcting the underlying sequellae: LLD and angular deformities
- These treatments may change in the future. Growth plate cartilage transplants and the use of stem cells may one day restore damaged sections of growth plates