The SUPERankle procedure was invented by Dr. Paley in 1996 (SUPER is an acronym for Systematic Utilitarian Procedure for Extremity Reconstruction). This procedure achieves a stable plantigrade (90°) foot and ankle that can be placed flat on the ground. It can be combined with lengthening but does not have to be. When there is a severe bend in the shaft of the tibia, correction depends on if lengthening happens concurrently with the SUPERankle. If the SUPERankle is combined with lengthening, the bend is corrected gradually with the lengthening using an external fixator. When there is no lengthening with the initial surgery, the bend is corrected by taking a wedge out of the bone and using internal pins and a cast. The lengthening will then be performed at a later date.
The decision to perform lengthening with the SUPERankle is determined by several criteria. If there is an extremely complex deformity, such that correction cannot wait until 18 months of age, Dr. Paley will perform a SUPERankle without lengthening. This is more commonly done in bilateral cases where limb length discrepancy is not a consideration. The other situation is when there is a well-developed ankle joint with excellent motion. There is a theoretical advantage in separating the SUPERankle procedure from the lengthening surgery to better preserve the ankle motion. The rationale for this is that performing the lengthening right away leads to increased stiffness of the ankle joint. If the ankle has excellent range-of-motion before surgery, performing the SUPERankle first to realign the foot and ankle, followed by physical therapy, will optimize the ankle range-of-motion. In theory, lengthening at this time could lead to a loss of ankle range-of-motion since the external fixator is on for a longer period of time and the muscles are tightened by the lengthening. This decision and discussion will be made with Dr. Paley at the time of the first consultation.
If the patient has an ankle with limited range-of-motion due to poor formation of the ankle joint shape (dysplastic ankle), they will not benefit from the two-stage SUPERankle and lengthening approach. In these cases, it is preferable to perform the deformity correction of the SUPERankle, combined with the lengthening, in order to decrease the total number of surgeries.
The first step of the SUPERankle procedure is to remove the fibrous fibular anlage. This remnant of the fibular bone tethers the lengthening and pulls the ankle and tibia into a valgus deformity (foot leaning to the outside). Removal of the anlage facilitates lengthening and prevents recurrent valgus.
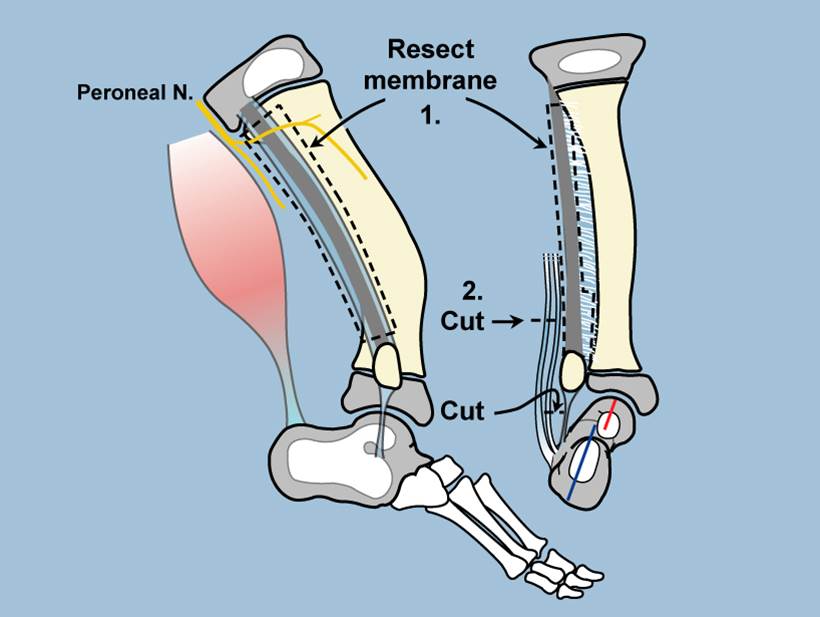
The second step of the SUPERankle is to lengthen the peroneal and Achilles tendons. Next, Dr. Paley will decompress the peroneal and posterior tibial nerves to prevent any damage to these structures from the deformity correction of the ankle. In highly dysplastic ankles, Dr. Paley will reshape the dome of the ankle bone (talus). Normally, the talus has a cylindrical shape to its joint surface. Dysplasia (malformation) of the talus leads to flattening of the cylindrical shape; furthermore, there is shortening of the front and back of the talus bone. This causes the front of the talus to bump into the front of the tibia when the foot is pulled up and the top of the heal bone to collide with the back of the tibia when the foot is pointed down. This leads to a very limited range-of-motion of the ankle joint. In 2009, Dr. Paley came up with a technique to reshape the talus and calcaneus bones to deepen the groove at the front and back of the ankle joint that permits the tibia to rock back and forth on the talus, thus increasing the range-of-motion of the ankle joint. This modification does not cause any harm, and there is no apparent downside to adding these groove deepenings as part of the SUPERankle procedure.
Type Details
Type 3A
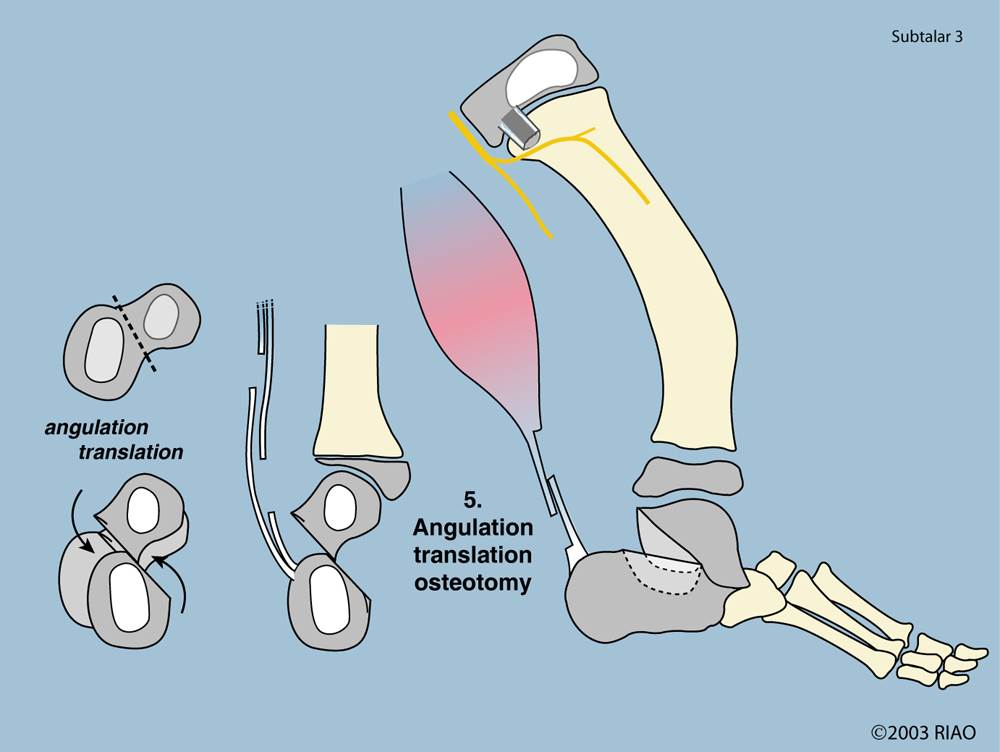
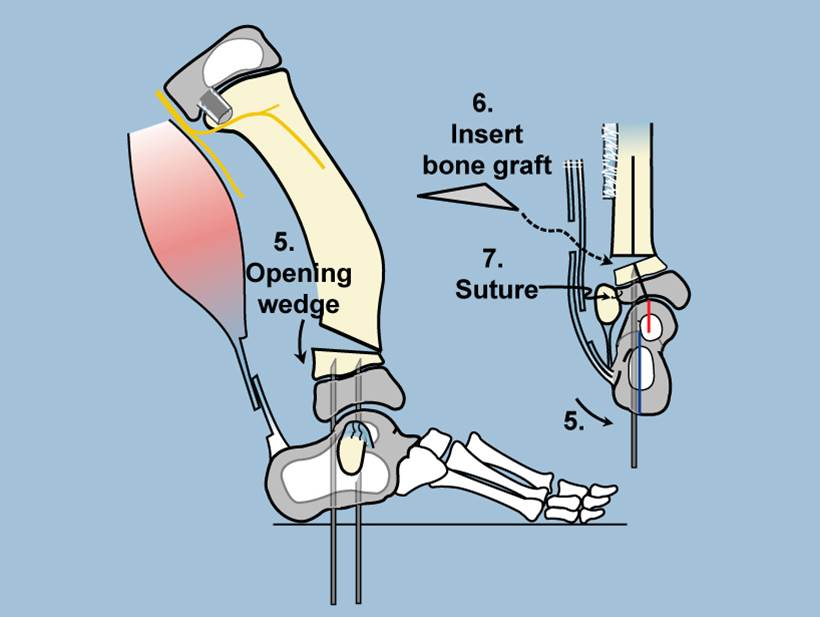
The next step of the SUPERankle is to perform the osteotomies. The specific osteotomy depends on the type of FH. In the Type 3A case, this involves a supramalleolar osteotomy of the tibia—bone cut above the ankle joint. Dr. Paley now performs a trapezoidal wedge rather than an opening wedge. A bone graft is then inserted. The bone graft is usually an allograft.
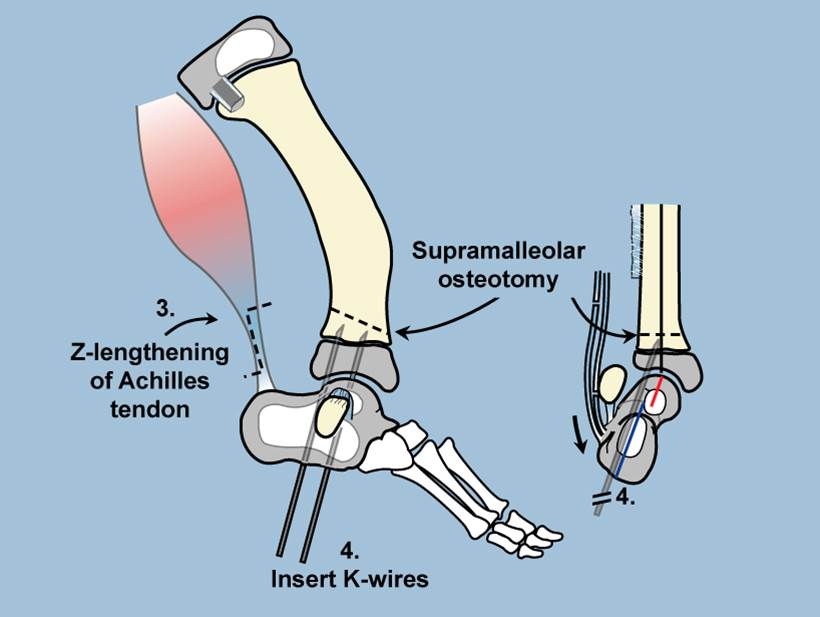
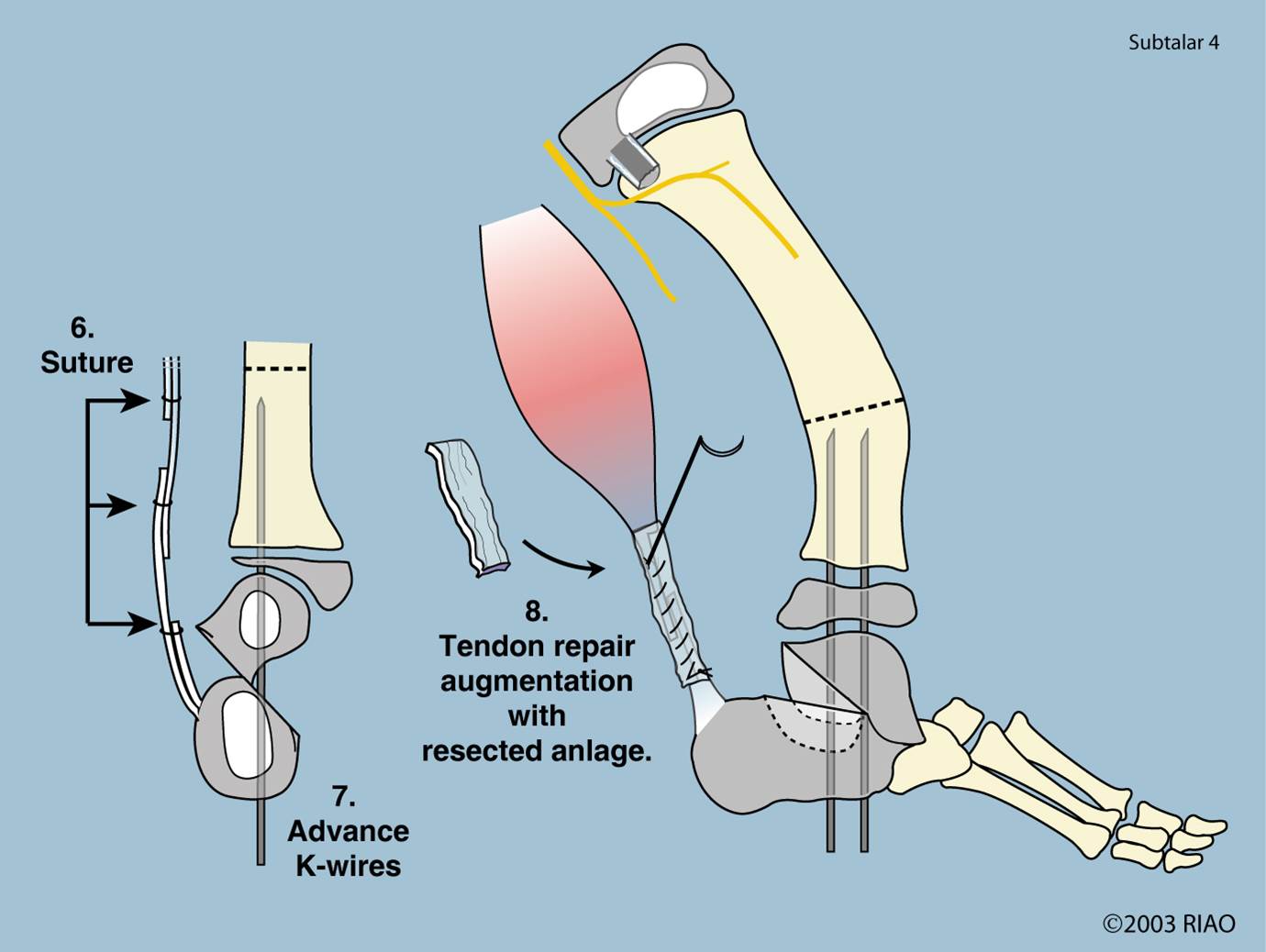
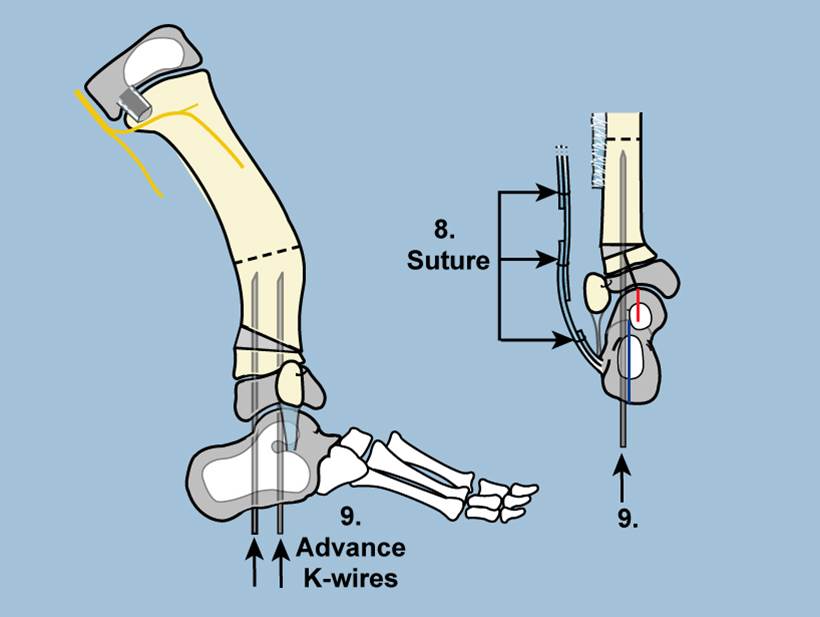
Dr. Paley will then fix the new ankle joint alignment in place with internal pins drilled through the heel pad and across the subtalar and ankle joints. The Achilles and peroneal tendons are then repaired. A compartment release is performed, which allows for swelling of the muscles within the leg.

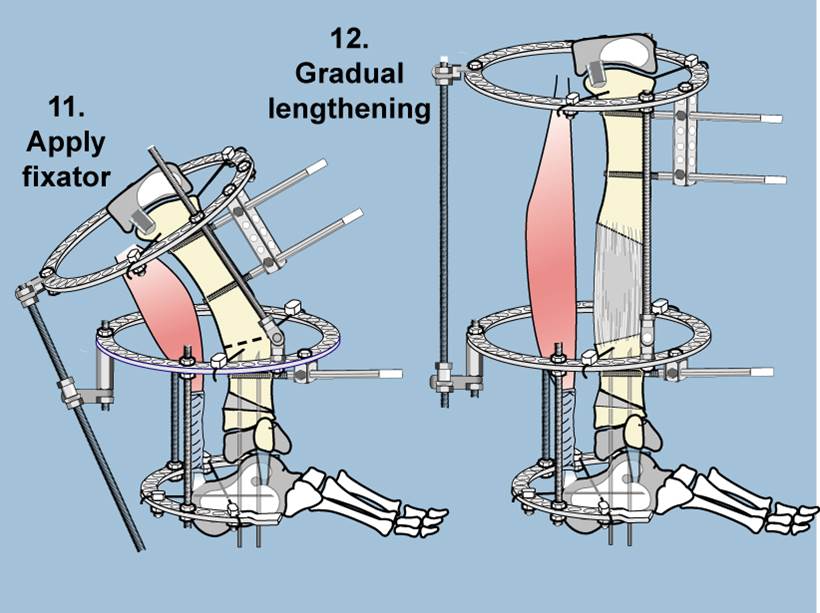
The final step of the SUPERankle will be applying an external fixator and cutting the bone at the apex of the tibial bend. As the lengthening occurs, straightening of the tibia is carried out by a gradual correction of the tibial bend using a computer-controlled external fixator called the Taylor Spatial Frame (TSF). The patient is given an adjustment schedule to start lengthening usually five to seven days after surgery.